Potential conflict of interest: Nothing to report.
Abstract
Severe
acetaminophen hepatotoxicity frequently leads to acute liver failure
(ALF). We determined the incidence, risk factors, and outcomes of
acetaminophen-induced ALF at 22 tertiary care centers in the United
States. Detailed prospective data were gathered on 662 consecutive
patients over a 6-year period fulfilling standard criteria for ALF
(coagulopathy and encephalopathy), from which 275 (42%) were determined
to result from acetaminophen liver injury. The annual percentage of
acetaminophen-related ALF rose during the study from 28% in 1998 to 51%
in 2003. Median dose ingested was 24 g (equivalent to 48 extra-strength
tablets). Unintentional overdoses accounted for 131 (48%) cases,
intentional (suicide attempts) 122 (44%), and 22 (8%) were of unknown
intent. In the unintentional group, 38% took two or more acetaminophen
preparations simultaneously, and 63% used narcotic-containing compounds.
Eighty-one percent of unintentional patients reported taking
acetaminophen and/or other analgesics for acute or chronic pain
syndromes. Overall, 178 subjects (65%) survived, 74 (27%) died without
transplantation, and 23 subjects (8%) underwent liver transplantation;
71% were alive at 3 weeks. Transplant-free survival rate and rate of
liver transplantation were similar between intentional and unintentional
groups. In conclusion, acetaminophen
hepatotoxicity far exceeds other causes of acute liver failure in the
United States. Susceptible patients have concomitant depression, chronic
pain, alcohol or narcotic use, and/or take several preparations
simultaneously. Education of patients, physicians, and pharmacies to
limit high-risk use settings is recommended. (HEPATOLOGY 2005;42:1364–1372.)
Acetaminophen,
the most widely used analgesic in the United States, causes severe
hepatic necrosis leading to acute liver failure (ALF) after suicidal
overdoses.1–3
Unintentional liver injury from self-medication for pain or fever that
leads to daily doses exceeding the 4 g/day package recommendations is
also well-recognized.4–7 Fasting and alcohol use may enhance toxicity, but this remains controversial.6, 8N-acetylcysteine
(NAC) can prevent hepatic injury if given within 12 hours of a single
ingestion. However, unintentional overdosing is usually only recognized
after symptoms have developed. Extended acetaminophen dosing, delay in
seeking medical attention, and/or failure to institute NAC therapy are
associated with greater morbidity and mortality.9, 10
In retrospective studies, poorer outcomes also have been reported for
subjects with unintentional acetaminophen overdose, but these data are
incomplete.4–7
Before the 1980s, acetaminophen was not mentioned as a cause in case series of ALF.11, 12 A U.S. retrospective study from 1994 to 1996 found a 20% incidence of acetaminophen toxicity leading to ALF.13
In January 1998, we began to examine prospectively the epidemiology and
outcomes of all forms of ALF in the United States at the centers
participating in the Acute Liver Failure Study Group (ALFSG). In the
current study, we investigated the incidence, risk factors, and outcomes
of a cohort of 275 consecutive U.S. patients with acetaminophen-related
ALF enrolled in the ALFSG registry over 6 calendar years from start of
study through December 31, 2003. Based on earlier observations, we
hypothesized that patients with unintentional acetaminophen overdose
would present with more severe disease [higher international normalized
ratio (INR), APACHE score, stage 3 or 4 encephalopathy], more frequently
suffer from alcohol abuse, and have a poorer rate of spontaneous
transplant-free survival compared with intentional overdose patients.14
Abbreviations
ALF, acute liver failure. NAC, N-acetylcysteine;
ALFSG, Acute Liver Failure Study Group; INR, International Normalized
Ratio; ALT, alanine aminotransferase; APACHE, Acute Physiology and
Chronic Health Evaluation II; MELD, Model for End-Stage Liver Disease;
OTC, over the counter; BMI, body mass index.
Patients and Methods
Between
January 1, 1998, and December 31, 2003, demographic, clinical,
laboratory, and outcome information were prospectively recorded on all
subjects meeting entry criteria for ALF at the 22 academic centers
participating in the ALFSG. By definition, eligible patients had an INR
≥1.5, evidence of hepatic encephalopathy,15 and presented within 26 weeks of illness onset without apparent chronic liver disease.13
Because subjects were encephalopathic (per definition), written
informed consent was obtained from their legal next of kin. Data were
collected on an admission case report form and subsequently on a
separate study outcome form, with outcome defined as liver
transplantation, discharge, or 3 weeks after admission.16
All centers were in compliance with their local institutional review
board requirements. A Certificate of Confidentiality was obtained from
the National Institutes for Mental Health for the entire study.
A
careful history of acetaminophen ingestion was elicited where possible
for each patient, including total dose, type of acetaminophen product
taken, and duration of use. Criteria for assigning acetaminophen as the
cause of ALF were: (1) a history of potentially toxic acetaminophen
ingestion (i.e., >4 g/day, the maximum dose recommended on
the package) within 7 days of presentation; (2) detection of any level
of acetaminophen in the serum; or (3) a serum alanine aminotransferase
(ALT) >1,000 IU/L with a history of acetaminophen ingestion,
irrespective of the acetaminophen level. Exclusion of competing causes
of ALF was also required, including acute hepatitis A and B, hepatic
ischemia, autoimmune hepatitis, and Wilson disease, among other
etiologies.16
Criteria for listing and proceeding with liver transplantation were
those used at each clinical center. Case report forms were reviewed by
investigators at the central site (UTSW) to confirm the diagnosis, and
annual on-site audits were conducted by the central site as well.
Definitions.
Patients
with ALF secondary to acetaminophen toxicity were assigned to one of
two groups by the local site investigator, according to the history
obtained: intentional (suicidal) ingestion—a single timepoint ingestion in a patient admitting suicidal intent; or unintentional ingestion—a multiple-timepoint ingestion to relieve pain or other somatic symptoms with denial of suicidal intent. Alcohol abuse
was defined as consumption of ≥40 g alcohol per day in men and ≥20 g
alcohol per day in women. The Acute Physiology and Chronic Health
Evaluation (APACHE) II score, Model for End Stage Liver Disease (MELD)
score, and the King's College Hospital criteria for ALF (“King's
Criteria”) were used to assess overall severity of illness at
presentation.17–19
Statistical Analysis.
Data are presented as medians, ranges, and percentages except where noted. In the analysis of the continuous data, the Student t
test or analysis of variance was used. In the analysis of nominal data,
the chi-squared test was used to examine differences between groups
when there were 2 or more possible values, and Fisher's exact test used
if the number of subjects in any group was under 10. All analyses were
two-tailed. P values of less than .05 were considered to indicate statistical significance.
Results
Overall Study Population
Of
the 662 ALF subjects enrolled during the 6-year study period, 302 (46%)
were reported to have acetaminophen-related hepatotoxicity.
Twenty-seven were excluded after further review: in 10, the most likely
cause was acetaminophen but data were insufficient and no other cause
was evident. In 17 patients, competing causes such as viral hepatitis,
concomitant polydrug use, or shock were identified. The remaining 275
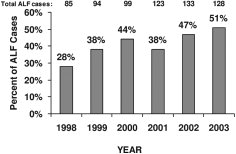
subjects (42%) constituted the final study group. Over the study period,
the percentage of ALF cases attributed to acetaminophen increased from
28% in 1998 to 51% in 2003 (Fig. 1).
The number and percentage of ALF cases attributed to acetaminophen for
the 6-year period far exceeded any other category, with 12% of cases
attributed to idiosyncratic drug-induced hepatotoxicity (prescription
drugs, herbs) and 19% considered indeterminate with no discernible cause
after complete evaluation.
Proportion
of ALF cases attributed to acetaminophen in each of the first 6 years
of the ALF Study Group: January 1998 to December 2003.
Criteria for Diagnosis
Of
the 275 subjects, 155 (56%) fulfilled the criterion of a history of
potentially toxic acetaminophen ingestion, 212 (77%) had detectable
acetaminophen levels in serum, and 250 (91%) had ALT ≥1,000 IU/L [ALT
was ≥3,500 IU/L in 160 (58%)]. One hundred eleven (40%) fulfilled all 3
criteria, 123 subjects (45%) fulfilled 2 criteria, and 37 subjects (13%)
fulfilled 1 criterion only. In 4 (1%), a history of toxic ingestion was
reported, but precise data on amount or level of acetaminophen were
lacking. However, all 4 of these subjects had elevated ALT levels when
they entered the study.
Clinical Presentation
A
total of 242 subjects (88%) had been transferred from an outlying
hospital. Subjects presented a median of 2.0 (range, 1–32) days after
the onset of symptoms and had ingested a median total dose of 24 g
(range, 1.2–180 g) of acetaminophen (Table 1).
The overall group was predominantly female (74%) and white (88%). Data
on volume of alcohol intake were available in 196 subjects, and 68 (35%;
25% of total group) met criteria for alcohol abuse.
Table 1. Features of Acetaminophen Overdose ALF Subjects; N = 275
Characteristic
Value
NOTE. Median (range) or numbers (%) are presented. Abbreviation: OTC, over-the-counter.
A
total of 147 subjects (53%) used only over-the-counter (OTC)
acetaminophen products; 141 (96% of this group) consumed only a single
OTC product, and 6 (4%) used two OTC products. A total of 120 subjects
(44%) reported ingestion of a prescription acetaminophen/narcotic
compound (e.g., Vicodin); 76 (28%) of 275 used these
combination products solely, and 41 (15%) used the prescription
combination product with OTC acetaminophen products. One hundred eight
subjects (39%) reported taking at least one prescription antidepressant,
and 34 (12%) reported taking either two or three prescription
antidepressants simultaneously. More females used antidepressants (46%
vs. 20% male; P < .0001), and antidepressant users were older [median, 39 years (range, 17–64) vs. 34 years (range, 17–76); P = .0018], and less likely to use (49% vs. 60%; P = .05) or abuse alcohol (24% vs. 40%; P = .02). Those taking antidepressants were also more likely to take additional prescription narcotics (17% vs. 5%; P = .003) and use acetaminophen/narcotic compound products (55% vs. 37%; P = .01). Antidepressant use was similar between the groups (37% vs. 38%).
Unintentional Versus Intentional Overdose
A
total of 122 subjects (44%) reported an intentional overdose, and 131
subjects (48%) experienced an unintentional acetaminophen overdose
without suicidal intent (Table 2).
In 22 (8%), the reason for the overdose was unclear. Subjects with
unintentional overdose were older (median, 38 years [range, 18–76]) than
those who attempted suicide (median, 32 years [range, 17–68]; P = .002), used multiple acetaminophen-containing preparations more frequently (38% vs. 5%; P
< .0001), and sought care longer after symptom onset (median 4 days
vs. 1 day). Unintentional overdose patients were less likely to report
depression (24% vs. 45%; P = .001). This group had significantly lower serum acetaminophen levels (16 μg/dL [range, 0–400] vs. 84 μg/dL [0–644]; P < .0001) and lower ALT levels (3,319 IU/L [range, 126–18,079] vs. 5,326 IU/L [179–19,826]; P
< .0001) at the time of admission to study. Unintentional patients
were more likely to have severe (grades 3 and 4) hepatic encephalopathy
on admission compared with the intentional overdose group (55% vs. 39%; P
= .002); however, the peak hepatic encephalopathy grade achieved during
the course of hospitalization and the number listed for transplantation
and time to transplantation did not differ between the groups. No other
clinical features differed between the 2 groups. History of past
substance abuse was similar between groups (unintentional, 35% vs.
intentional, 31%; P = .11). Toxicology screens (all drugs of
abuse, including narcotics) were available in 77 subjects (28%) and
positive in 58 (21%). Among the 58 with positive screens were 10
positive for marijuana, 11 for cocaine, and 5 for amphetamines. The
remainder were positive for opiates, benzodiazepines, barbiturates, or
tricyclic antidepressants or combinations thereof, most of which likely
represented prescribed medications. The educational level was similar
between the unintentional (mean, 12.97 years) and intentional (13.26
years) groups, and these were similar to that seen in the ALF patients
as a whole (13.22 years) and to those with drug-induced liver injury
from other causes (13.53 years).
Table 2. Baseline Features/Outcomes in Intentional and Unintentional Acetaminophen Overdose
Characteristic
Unintentional Overdose (N = 131)
Intentional Overdose (N = 122)
Value
No. of Patients Included
Value
No. of Patients Included
NOTE.
Median (range) or numbers (%) are presented. 22 subjects could not be
classified as suicidal or accidental. Data available for all 275
subjects except as noted (n = xxx).
Nineteen
patients with unintentional overdose reported that they had used
acetaminophen for more than 7 days. This chronic use group was older,
weighed more, reported larger total acetaminophen ingested, was more
likely to report pain as the reason for use, was less likely to use
alcohol, and was more likely to take additional narcotics. This group
otherwise did not differ from those who used acetaminophen for fewer
than 7 days in any other measurement.
Prescription Acetaminophen/Narcotic Compound Use
Use
of prescription narcotic/acetaminophen compounds (“compounds”) was
reported by 120 (44%) of the entire group of patients studied and was
primarily observed in the unintentional group (63% vs. 18% for the
intentional group; P < .0001). The product most commonly
used was Vicodin (acetaminophen/hydrocodone, Abbott Laboratories,
Chicago IL; n = 83 of 120). Clinical indicators of disease severity such
as platelets, serum ALT, and bilirubin were significantly lower in the
compound users. However, other indicators, including transplantation
rate and overall survival, did not differ between the compound users and
remaining subjects.
Alcohol Use and Abuse
Those
who chronically used or abused alcohol constituted 55% and 35%,
respectively, of the entire group. Compared with nonabusers, alcohol
abusers had lower acetaminophen levels (15 μg/dL [range, 0–315] vs. 34
μg/dL [0–644]; P = .003), were less likely to use antidepressants (24% vs. 40%; P = .03) or compound narcotics (31% vs. 50%; P = .009), and were less likely to present with severe (grades 3 and 4) hepatic encephalopathy (34% vs. 53%; P
= .02). Clinically, there were no other differences between those who
were abstinent and those who abused alcohol with regard to INR, ALT,
bilirubin, body mass index (BMI), APACHE II score, MELD score, or
overall survival (data not shown).
Ingestion of Low Doses of Acetaminophen: ≤4 Grams/Day
Nineteen
(7%) subjects reported taking ≤4 g acetaminophen per day before
presentation. Sixteen had ALT levels over 1,000 IU/L (range for the
entire group: 136–11,240), and 12 had measurable serum acetaminophen
levels. Compared with the remaining subjects ingesting higher doses, the
low-dose group was older (median, 46 vs. 34 years; P = .01), more often reported unintentional overdose (74% vs. 40%; P < .002), and more often used (79% vs. 59%; P = .09) or abused (65% vs. 37%; P
= .02) alcohol. The low-dose group displayed slightly lower serum
acetaminophen levels (median, 14.5 μg/dL [range, 0–383] vs. 31 μg/dL
[0–315]) and elevations in serum ALT (median, 2,949 IU/L [range
175–19,826] vs. 4,224 IU/L [136–11,240]); however, these differences
were not statistically significant. All other measures were similar
between the low- and higher-dose groups.
Outcome and Predictors of Spontaneous Survival
Overall,
178 subjects (65%) survived without liver transplantation; 74 (27%)
died, and 23 subjects (8%) underwent transplantation. Seventy-two
subjects (26%) were listed for transplantation: 20 died and 29 recovered
without receiving an organ. Overall, 196 subjects (71%) were reported
to be alive at the 3-week outcome point.
Spontaneous Survival.
The 178 nontransplanted survivors were less ill at presentation than the nonsurvivors (Table 3).
Although spontaneous survivors were more likely to have abused alcohol,
there were no significant differences in sex, age, ethnicity, type of
overdose, total acetaminophen dose, serum acetaminophen level,
antidepressant use, narcotic or narcotic compound use, bilirubin,
platelets, temperature, or BMI at presentation between the groups (data
not shown).
Table 3. Comparison of Spontaneous Survivors and Nonsurvivors (Death or Transplant)
Characteristic
Died or Transplantation (N = 97)
Survival Without Transplantation (N = 178)
P Value
NOTE. Median (range) or numbers (%) are presented. Data were available for all 275 subjects except as noted (n = xxx).
Age (years)
38 (18–76)
36 (17–68)
.68
Chronic alcohol use (n = 273)
48 (50%)
103 (58%)
.21
Chronic alcohol abuse (n = 196)
15 (24%)
53 (39%)
.04
NAC treatment received
90 (93%)
162 (91%)
.82
Admission hepatic coma grade (n = 271)
4 (1–4)
2 (1–4)
<.0001
Admission hepatic coma (stages 3–4)
75 (77%)
60 (34%)
<.0001
Peak hepatic coma grade (n = 273)
4 (1–4)
2 (1–4)
<.0001
Peak hepatic coma (stages 3–4)
96 (99%)
84 (47%)
<.0001
Met Kings criteria (% yes)
25 (26%)
15 (8%)
<.0001
APACHE II score (n = 216)
22.5 (8–40)
14 (2–31)
<.0001
Apache II score >15 (% yes)
78 (93%)
60 (45%)
<.0001
MELD score (n = 268)
36 (11–53)
28 (7–52)
<.0001
Systolic blood pressure (n = 274)
117 (64–188)
129 (77–191)
.005
Heart rate (beats per minute) (n = 273)
116 (65–156)
99 (53–145)
<.0001
White blood cells (thousands) (n = 273)
12.4 (1.6–49.8)
9.1 (1.4–25.6)
.0002
INR (n = 269)
3.8 (1.3–27.1)
2.8 (1.2–24.1)
.004
ALT (n = 274)
4,429 (136–19,826)
4,030 (158–15,120)
.05
Creatinine
2.7 (0.2–9.2)
1.4 (0.4–10.5)
.0003
Arterial pH (n = 246)
7.38 (6.94–7.67)
7.44 (7.0–7.9)
.01
Use of King's Criteria.
The
King's criteria for liver transplantation were fulfilled on admission
in only 40 subjects, of whom 19 died without transplant and 6 underwent
transplantation (2 died and 4 were alive at 3 weeks).18
Of 235 subjects who did not meet the King's criteria, 163 subjects
survived without a transplant, 55 died without receiving a transplant,
and 17 subjects underwent liver transplantation (3 of whom died and 14
were alive at the 3-week outcome timepoint), yielding a low sensitivity
and high specificity (Table 4).
Table 4. Comparison of Sensitivity, Specificity, and Positive and Negative Predictive Values of Two Prognostic Systems
Sensitivity
Specificity
Positive Predictive Value
Negative Predictive Value
Percent Correct
Likelihood Ratio
Kings (≥ 1)
26%
92%
63%
69%
68%
3.06
APACHE II (≥ 20)
68%
87%
77%
81%
80%
5.27
Use of the APACHE II Score.
The
APACHE II score assessing overall severity of illness on admission was
available in 216 subjects and was divided into 2 groups (low at <20
and high at ≥20), based on a receiver operator characteristic curve
(data not shown).17
Subjects with an APACHE II score of ≥20 had a significantly lower
transplant-free survival than subjects with a score of <20 (43% vs.
92%, P < .0001) and more often underwent transplantation (13% vs. 1%; P = .002); this yielded a much higher sensitivity but slightly lower specificity than the King's criteria (Table 4).
Discussion
Acetaminophen poisoning has become the most common cause of ALF in both the United States and the United Kingdom.13, 20–22 Underreporting may have occurred in the past when transplant databases were used.13, 22
Nevertheless, current data suggest a dramatic increase in acetaminophen
toxicity recently; the percentage of all ALF cases in our registry that
were due to acetaminophen has nearly doubled in 6 years. Although they
are less frequent in terms of overall acetaminophen-related
hospitalizations, unintentional overdoses constitute at least half of
all those that develop encephalopathy.7
Intentional and unintentional cases have similar clinical pictures and
outcomes once the threshold of ALF has been reached. In many subjects,
multiple factors appear to be at play, including repeated dosing in
excess of package labeling, use of multiple acetaminophen-containing
products, simultaneous use/abuse of alcohol and narcotics, and
depression. Patients with chronic pain appear to be particularly
susceptible to this problem.
Although our study included
consecutive subjects studied prospectively, it has several limitations.
First, we portray here only the most severely ill subjects who meet
criteria for ALF.7
In addition, our group may not represent the true incidence of ALF in
the population at large, because many patients are not referred to
transplant centers because of failure to diagnose ALF, presumption of
mild disease, suicide or substance abuse histories, poor prognosis
(cancer patients, the elderly), or unsuitability for liver
transplantation.14
Our patients were evaluated by experienced hepatologists, and the
history of all drug and alcohol ingestion was determined carefully.
Nevertheless, patients by definition have altered mentation, making
accurate history-taking difficult or impossible. For example, obtaining a
recent food or alcohol intake history immediately before
hospitalization was not feasible. More than 80% of patients were
transferred from other institutions, often after significant
encephalopathy had set in, compromising history (i.e., time of last dose, total dose ingested, etc.).
Our
study sites, representing approximately 30% of U.S. transplant
capability (United Network for Organ Sharing data), recorded an average
of 49 acetaminophen-related liver failure cases/year over the 6-year
period. Based on data from site enrollment logs, an additional 40% of
cases were not enrolled because of lack of informed consent or
inadequate information to ensure the diagnosis (data not shown). Thus,
we estimate that at least 250 cases of acetaminophen-related ALF are
seen annually at U.S. transplant centers, resulting in approximately 73
deaths. This is considerably less than the estimated 458 deaths per year
attributable to acetaminophen poisoning predicted by the FDA, possibly
reflecting lack of referral for transplant of suicidal or
substance-abuse patients. Nevertheless, a high proportion of our
patients who were referred to a transplant center demonstrated substance
abuse or major psychiatric problems. Of interest, data from a large
national survey suggest that 36% of Americans ingest an
acetaminophen-containing compound at least once a month; this figure
underscores the low incidence of ALF due to acetaminophen overdose
compared with the millions of tablets consumed on a daily basis.23
One
of the most alarming findings in our study was that unintentional
acetaminophen overdose accounted for 50% of our cases. The rate of
unintentional overdose was estimated to be 31% in Australia, and
nonsuicidal overdoses are only rarely reported in the United Kingdom and
Europe.24–26 Single timepoint ingestions with suicidal intent constituted 70% of all hospitalized
subjects in one U.S. series, but these subjects frequently presented
early after ingestion when use of NAC would be effective, so that few
developed encephalopathy and only 2% died.7
In the current series, in which cases were limited to those subjects
reaching the threshold of encephalopathy, the mortality rate was higher
(approximately 29%) and similar for the intentional and unintentional
groups. Whereas unintentional cases uniformly present after symptoms
have developed, those with suicidal intent who develop encephalopathy
typically have other cofactors such as use of alcohol, narcotics, or
sedatives that may delay presentation or enhance toxicity.
We have
been careful to describe the features of the unintentional group
because their incidence differs markedly from the experience in other
countries. Amongst unintentional overdose patients, most (79%) reported
that they were taking the medication(s) specifically for pain or
constitutional symptoms (8%). Many claimed to have ingested modest
amounts of acetaminophen over weeks or months, with 63% reporting use of
narcotic combinations.4, 6, 27–29
Why, then, the sudden onset of severe liver injury? Our data suggest
that there is a narrow therapeutic margin and that consistent use of as
little as 7.5 g/day may be hazardous. However, precise information on
dosing is often difficult to acquire in some of these patients. We are
planning to look at this issue in more detail in a future study. Late
presentation is undoubtedly a factor in the unintentional cases as
described in this study and previously,7
but the acuity of the unintentional cases (height of ALT levels,
severity ofillness) was similar to single timepoint ingestions. The
development of tolerance to gradually increasing doses of acetaminophen
has been reported previously in association with narcotic abuse.27
Worsening pain may occasion the supra-normal dosing in the days before
admission. Alternatively, loss of tolerance may result from alcohol use,
starvation, or inter-current illness leading to glutathione depletion.6
In spite of long-term ingestion histories, the cases that reported
>7 days' ingestion still had an acute injury, in terms of their
biochemical values, that was indistinguishable from suicidal ingestions,
suggesting that there is no chronic form of injury, but rather a
threshold of safety that may be breached with devastating results.
Toxicological testing, while performed in a limited number of patients,
strongly suggested use of illicit drugs, although the information
available included illegal as well as legal narcotic use. There was no
impact observed for lower socioeconomic groups in the acetaminophen
group because no difference in level of education was evident between
the acetaminophen groups and other forms of ALF. Some may have had
genetic polymorphisms making them more susceptible to acetaminophen
poisoning at lower doses, but most had ingested doses that would be
expected to cause severe liver injury.30, 31
A
second potential reason for toxicity is the simultaneous use of 2
preparations, recorded in 22% overall, and 38% of the unintentional
group. Information was not available regarding the reason for the use of
2 preparations, but frustration, impulsivity, or simply lack of
recognition of the presence of acetaminophen in both preparations have
all been recognized.32
Of interest, a third of narcotic users were simultaneously ingesting an
over-the-counter acetaminophen product (data not shown). This suggests
patients' lack of awareness of the hazards of over-the-counter
acetaminophen use in combination with prescribed agents.32
An independent interview evaluation after patients have recovered might
help in establishing exact dosages, reasons for excess ingestion, and
patient understanding of the implications of overdosing on this
ubiquitous but hazardous medication.33
A full third of our subjects met standard criteria for alcohol abuse (i.e.,
>40 g/day in men and >20 g/day in women). These subjects less
often used acetaminophen/narcotic compounds or antidepressants,
suggesting that they may have been self-medicating with alcohol. Their
acetaminophen levels were lower, despite reporting intake of similar
amounts of acetaminophen. Because the subjects with ALF reporting use of
≤4 g acetaminophen per day were often alcohol abusers (65%) and the
amount of daily alcohol consumed was greater than that reported by
patients who admitted to taking >4 g acetaminophen per day (data not
shown), ethanol may still serve as an important co-factor in these
lower-dose subjects.4, 6, 13, 24, 34–36
The
overall transplant-free survival rate of 65% in acetaminophen subjects
is comparable to that of prior studies and continues to be more
favorable than that observed for most other ALF causes.13, 37, 38, 39
The use of the King's criteria at admission to predict outcome was
inaccurate, and use of the APACHE II provided a more accurate of
assessment outcome. Clearly, improved prognostic criteria are needed.22, 39, 40
In
conclusion, acetaminophen poisoning now accounts for at least 42% of
U.S. acute liver failure cases seen at tertiary-care centers and one
third of the deaths. Unintentional overdose is the leading form of
acetaminophen hepatotoxicity in U.S. ALF subjects, but suicidal
ingestions remain important as well. Susceptible patients include those
with chronic pain, depression, and substance abuse, including alcohol.
Legislative changes in the United Kingdom leading to restrictions in the
sales of acetaminophen have reduced the number of patients dying from
or needing transplantation because of acetaminophen hepatotoxicity.33, 41–46
Because most cases in the United Kingdom are considered to be suicidal,
they differ in that sense from unintentional cases. Nevertheless,
efforts to limit OTC package size and to restrict the prescription of
narcotic–acetaminophen combinations (or to separate the narcotic from
the acetaminophen) may be necessary to reduce the incidence of this
increasingly recognized but preventable cause of ALF in the United
States. Educational programs for practicing physicians, pharmacists, and
consumers, involving a full discussion of the hazards of this
ubiquitous pain reliever and the identification of susceptible groups,
seems warranted.
Acknowledgements
The authors thank all the nurses, investigators, and house staff who tirelessly work to make this study possible.
Appendix
The Acute Liver Failure Study Group 1998–2003:
William
M. Lee (PI), Julie Polson, Ezmina Lalani, Frank V. Schiødt, George
Ostapowicz, Linda S. Hynan, Joan S. Reisch, University of Texas
Southwestern Medical Center, Dallas, TX
Anne M. Larson, Hao Do, University of Washington, Seattle, WA
Jeffrey S. Crippin, Laura Gerstle, Washington University School of Medicine, St. Louis, MO
Timothy J. Davern, Nathan Bass, Lily Luu, University of California at San Francisco, CA
Michael Schilsky, Jeanna Zalsos, Mt Sinai Medical Center, New York, NY
Timothy M. McCashland, Tamara Bernard, University of Nebraska, Omaha, NE
J. Eileen Hay, Cindy Groettum, Mayo Clinic, Rochester, MN
Natalie Murray, Sonnya Coultrup, Baylor University Medical Center, Dallas, TX
A. Obaid Shakil, Diane Morton, University of Pittsburgh Medical Center, Pittsburgh, PA
Andres T. Blei, Jeanne Gottstein, Northwestern University Medical School, Chicago, IL
Atif Zaman, Renee Rutledge, Oregon Health Sciences University, Portland, OR
Steven Han, Val Peacock, University of California at Los Angeles, CA
Robert J. Fontana, Nadia Tayeh, University of Michigan Medical Center, Ann Arbor, MI
Brendan McGuire, Pam Davis, University of Alabama, Birmingham, AL
Raymond Chung, Deborah Casson, Massachusetts General Hospital, Boston, MA
Robert Brown Jr., Laren Senkbeil, Columbia-Presbyterian Medical Center, New York, NY
M. Edwyn Harrison, Rebecca Rush, Mayo Clinic, Scottsdale, AZ
Adrian Reuben, Nancy Huntley, Medical University of South Carolina, Charleston, SC
Santiago Munoz, Chandra Misra, Albert Einstein Medical Center, Philadelphia, PA
Todd Stravitz, Jennifer Salvatori, Virginia Commonwealth University, Richmond, VA
Lorenzo Rossaro, Katherine Suggett, University of California, Davis; Sacramento, CA
Raj Satyanarayana, Wendy Taylor, Mayo Clinic, Jacksonville, FL




{kind=link}